This the protocol for a Peritonsillar Abscess:
Let’s break it down!

Classically known as a “Quinsy”, a peritonsillar abscess is an abscess that is located along the tonsillar pillars. It’s typically a complication of tonsillopharyngitis, which is inflammation of tonsils and pharynx due to a viral or bacterial pathogen. If the tonsillopharyngitis is caused by streptococcus bacteria, it’s commonly referred to as “Strep Throat”. More often than not, a peritonsillar abscess will follow streptococcal pharyngitis as opposed to a viral one. About 3 per 10,000 people are affected every year, with young adults most commonly affected. For soldiers, this is something you should always be highly suspicious for any time they come to you with a sore throat.
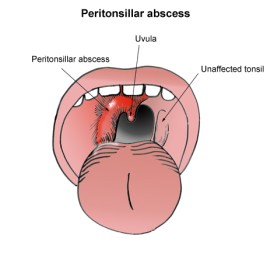

A patient who walks in with a peritonsillar abscess is generally going to be in more pain than your simple strep throat patient, and the pain will typically localize more on the affected side. The abscess can develop enough to cause neck pain, asymmetry of the oropharynx, dysphagia (difficulty swallowing), etc. As with any infection, a fever can also be suspected as well. Due to the swelling, some patients may even have a “hot potato voice“. If you don’t know what that sounds like, check out the video:
Here’s another quick video by Dr.ER. that show’s a simple case tonsillopharyngitis WITHOUT a peritonsillar abscess
And this is a case of tonsillopharyngitis WITH a peritonsillar abscess:

Although we can definitively say whether or not the abscess is caused by a viral or bacterial agent, we typically just assume the most likely scenario in that it is bacterial. Plus, any head/neck infection has the potential for severe complications. So step 1: give antibiotics!
Which antibiotic should you give? Any antibiotic that covers Streptococcus, Staphylococcus, and anaerobes is a solid choice. Clindamycin, Amoxicillin/Clavulanic Acid, and Ceftriaxone are all broad-spectrum antibiotics that cover these agents.



For obvious reasons, the patient is going to need pain management. A short course of NSAIDs and/or Tylenol from the Pain Management protocol should suffice.
Although not mentioned in the protocol, steroids like Dexamethasone and Methylprednisolone are also commonly used to reduce the amount of inflammation in the throat. Not a lot of great data to support this practice, but it may reduce pain and prompt a faster recovery.
![]()
Like any abscess, drainage is key for recovery. Some evidence even suggests that drainage alone w/o antibiotics may be a feasible treatment option. Needless to say, it’s going to be an important part of treatment if the abscess does not resolve on its own throughout the course of antibiotics.
Although draining these abscesses aren’t quite in our scope of practice, here are some good videos on how to do it (just in case you’ve got a cool PA):

Regardless of our treatment, these patients are going to get at least a Routine evacuation. Drainage is a key part of treatment for many of these patients and even emergency physicians are hesitant to perform a drainage w/o an ENT specialist. There’s always a possibility that the abscess can become large enough to compromise the airway, which certainly prompts at least a Priority evacuation.
With early and appropriate treatment, most peritonsillar infections resolve without any major complications. Symptoms should disappear between 5-7 days. Recurrence is estimated to occur in about 10 to 15 percent of patients, which is why some patients will opt to have their tonsils removed later on.
Till next time!
References
- EMRAP Corependium: Pharynx and Throat Emergencies
- Chau JK, Seikaly HR, Harris JR, Villa-Roel C, Brick C, Rowe BH. Corticosteroids in peritonsillar abscess treatment: a blinded placebo-controlled clinical trial. Laryngoscope. 2014;124(1):97–103. doi:10.1002/lary.24283
- Powell J, Wilson JA. An evidence-based review of peritonsillar abscess. Clin Otolaryngol. 2012;37(2):136–145. doi:10.1111/j.1749-4486.2012.02452.x
- Advanced Tactical Paramedic Protocols Handbook. 10th ed., Breakaway Media LLC, 2016.